Overview
Chronic pain is defined as pain that persists beyond the usual course of recovery from acute illness or injury (often > 3 months). Chronic pain is a complex syndrome with physical, psychological, social, and emotional components, which may result in sleep disorders, social isolation, and/or overall loss of function. Unfortunately, the management of chronic pain focuses on analgesia, which can be difficult to achieve, while neglecting chronic pain’s whole person health impact.2
Primary care providers (PCPs) prescribe more opioids than any other group of providers.3 Evidence supporting the efficacy of opioids is inconclusive and suggests that chronic opioid therapy (COT) may not improve function. However, strong and conclusive evidence demonstrates the harms of opioids.4,5 Out of the estimated 10-12 million American adults receiving COT6, approximately 2 million misuse, abuse, or are addicted to prescription opioids, including approximately 25% of those receiving COT for non-cancer pain. According to the most recent statistics, 115 Americans die each day from prescription opioid overdose.7 This is such a serious issue that in May 2018, the FDA Commissioner suggested mandating opioid education for physicians.8
This document focuses on chronic non-cancer pain (referred to as “chronic pain”) in adults with an emphasis on the safe and effective use of opioids. This document does not apply to patients with pain from an acute injury, post-operative recovery, cancer pain, degenerative major joint disease, headache syndromes, neuralgias of the head or face, or pain management needs at the end of life. Guidelines on chronic pain vary in scope and recommendations; however, they share the common challenge of relying on evidence of limited quality. Guidelines differ on the following factors: use of screening tools, doses, use and frequency of urine drug screens, opioid rotation, use of specific opioids (e.g., fentanyl). As a result, many of the recommendations throughout this document have lower levels of evidence as compared to other ACT documents.
Figure 1. Assessment and Management of Chronic Non-Cancer Pain
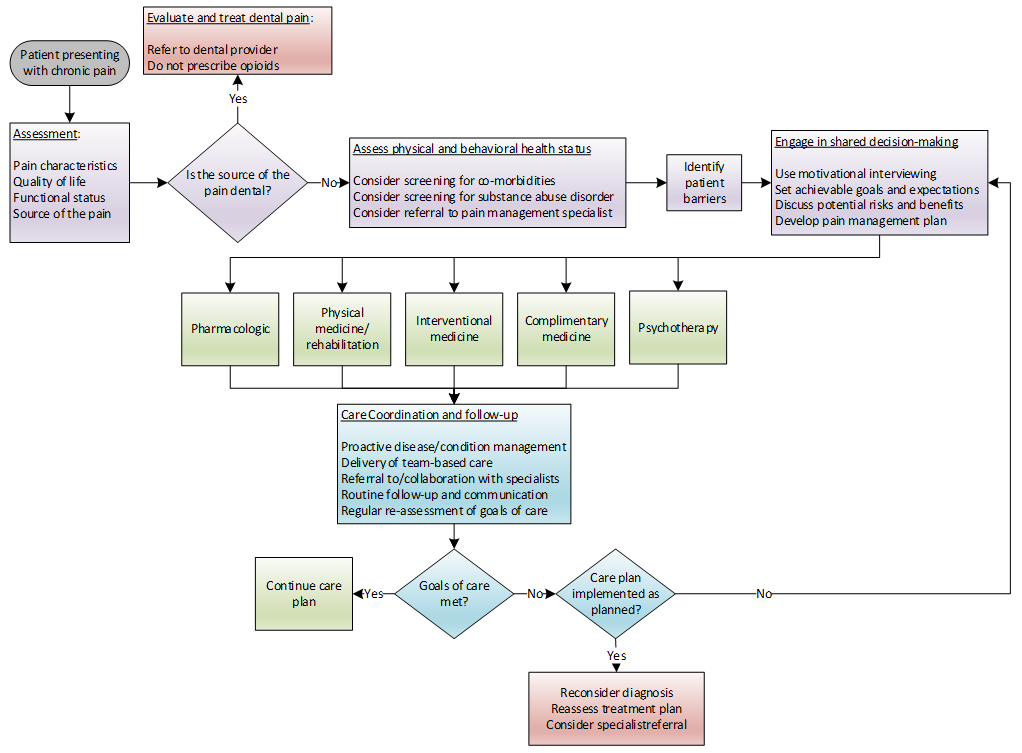
Adapted from:
Hooten M, Thorson D, Bianco J, et al. Pain: Assessment, Non-Opioid Treatment Approaches and Opioid Management. URL: https://www.icsi.org/guidelines__more/catalog_guidelines_and_more/catalog_guidelines/catalog_neurological_guidelines/pain/. Updated: August 2017. Accessed: June 22, 2020.
Key Points
Standard of Care Recommendations| Assessment Recommendations | |
| Treatment Recommendations |
Lumeris’ Most Important Considerations
| Psychotherapy and regular exercise should be considered in all patients with chronic pain | |
| Pharmacotherapy should be used as an adjunct to non-pharmacological treatments for chronic pain | |
| Due to an excessive risk of addiction and death compared to modest benefits, opioid therapy should generally be avoided for the treatment of chronic non-cancer pain | |
| Elderly patients who receive opioid prescriptions from multiple prescribers may be at higher risk of opioid-related hospitalization. | |
| Periodically evaluate the benefits and harms of opioid therapy and proactively prevent opiate-related harms | |
| Elderly patients who receive opioid prescriptions from multiple prescribers may be at higher risk of opioid-related hospitalization. | |
| Misunderstanding and misapplication of opioid restrictions intended for opioid-naïve patients can lead to harm in opioid-dependent patients | |
| Consider referring patients with signs of inappropriate opioid use to an addiction specialist. | |
| Department of Health and Human Services recommends tapering and discontinuation of long-term opioids in select patients who may benefit. |